
Non-paraneoplastic antibodies
This group of antigens are directly accessible to circulating antibodies (considered pathogenic) due to their extracellular location (i.e. neuronal cell surface) and are responsive to treatment.
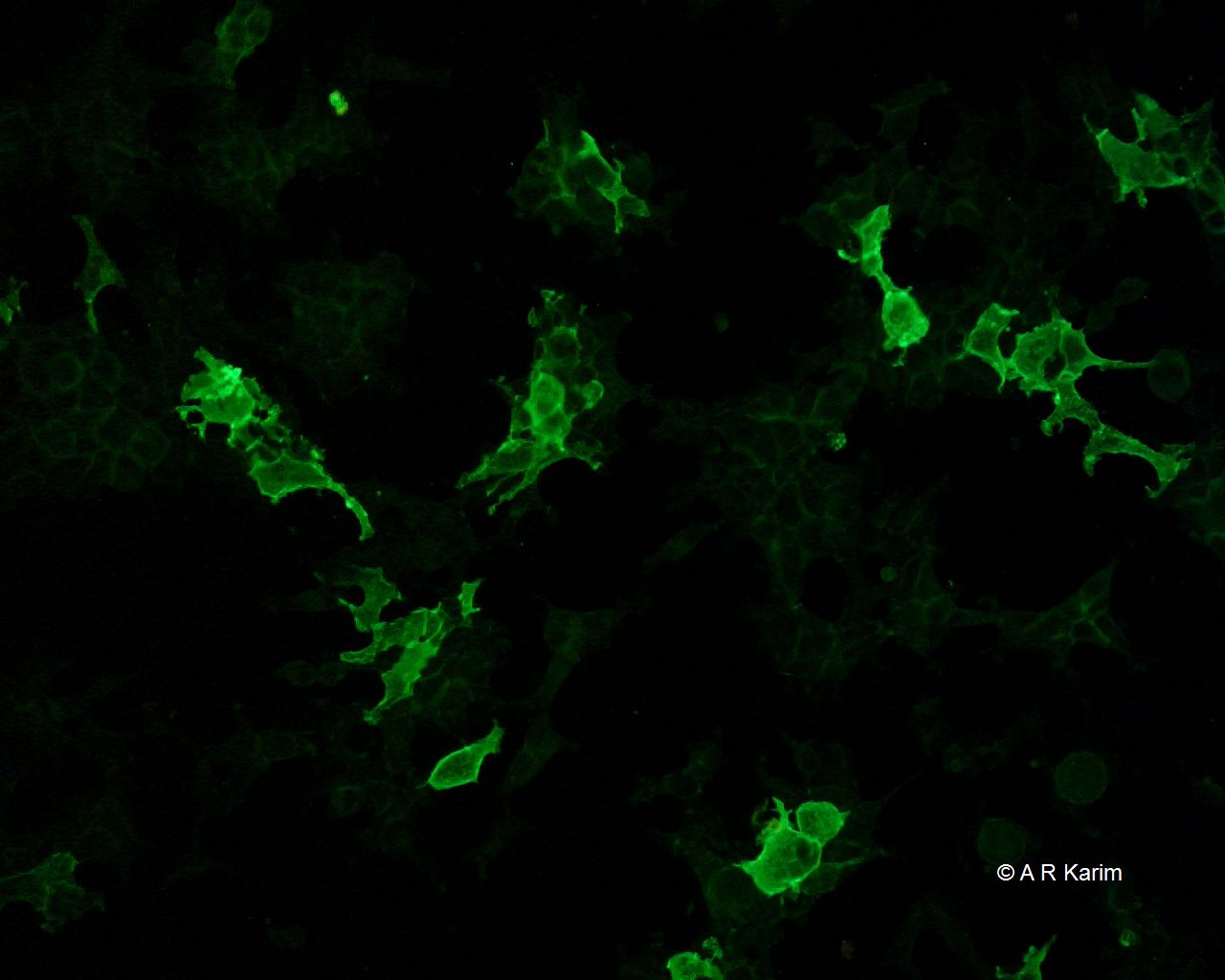
These antibodies are detected by the staining seen on the transfected HEK cells.
Some of these include the following:-
| Antibody | Antigen | Neurological Disorder | Associated tumour(s) | Target antigen |
| NMDAR | Glutamate receptor | LE | Ovarian teratoma | N-terminal extracellular domain of the NR1 subunit of NMDAR |
| LG1 | VGKC protein | LE with FBDS | Rare | LGI1 |
| CASPR2 | VGKC protein | Neuromyotonia | + / - | CASPR2 |
| APAR | Receptor | LE | + / - Lung, breast or thymus | GluR1 and GluR2 subunits of AMPAR |
| GABABR | Receptor | LE (mainly seizures) | SCLC | B1 receptor subunit of GABABR |
| Glycine | Receptor | PERM | Rare | α1 receptor subunit of Glycine receptor |
Abbreviations
AMPAR - alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor, CASPR2 = contactin-associated protein-like 2, GABA – Gamma amino butyric acid, LGI1 = Leucine-rich glioma-inactivated protein 1 antibody, SOX = Sex determining region Y-box,
FBDS = Faciobrachial-dystonic seizures, LE = limbic encephalomyelitis, PERM = Progressive encephalomyelitis, with rigidity and myoclonus
VGKC = Voltage gated potassium channel,
HEK = Human Embryonic Kidney
Overview of Non-Paraneoplastic Antibodies
Anti-glial nuclear antibody (AGNA) antibodies
Anti-glial nuclear antibody (AGNA) antibodies
AGNA or SOX1 antibody is directed against the Bergmann glia of the Purkinje cell layer of cerebellum. It has been described in patients with PNS (usually Lambert Eaton myasthenic syndrome) associated with SCLC. The target for this antibody is SOX1 & SOX2 protein with higher positivity seen against SOX1.
Clinical case
Patient details
- 79yr old lady, admitted with right sided chest pain
- Weight loss over the past few months.
- Swallowing difficulties
Work-up
- A chest X-ray on admission revealed a right sided lesion
- CT thorax/abdomen revealed a large mass in the posterior mediastinum
- Extensive metastases noted within the chest and abdomen
If SOX1 antibodies are found, they are highly predictive of a small cell lung cancer and extensive tumour screening should be undertaken (including repeat imaging, PET scans etc.), even if the initial scans are apparently normal.
NMO (aquaporin 4) antibodies
NMO (aquaporin 4) antibodies
Neuromyelitis optica (NMO) associated antigen, a water channel protein, known as aquaporin 4 (AQP4) is found both in the central and peripheral tissues. Detection of AQP4 antibody is clinically useful in differentiating between NMO and other optic neuritis or myelitis.
On cerebellum, AQP4 is found in the juxtaposed pial membrane, microvessels in the white matter, molecular layer and granular layer.
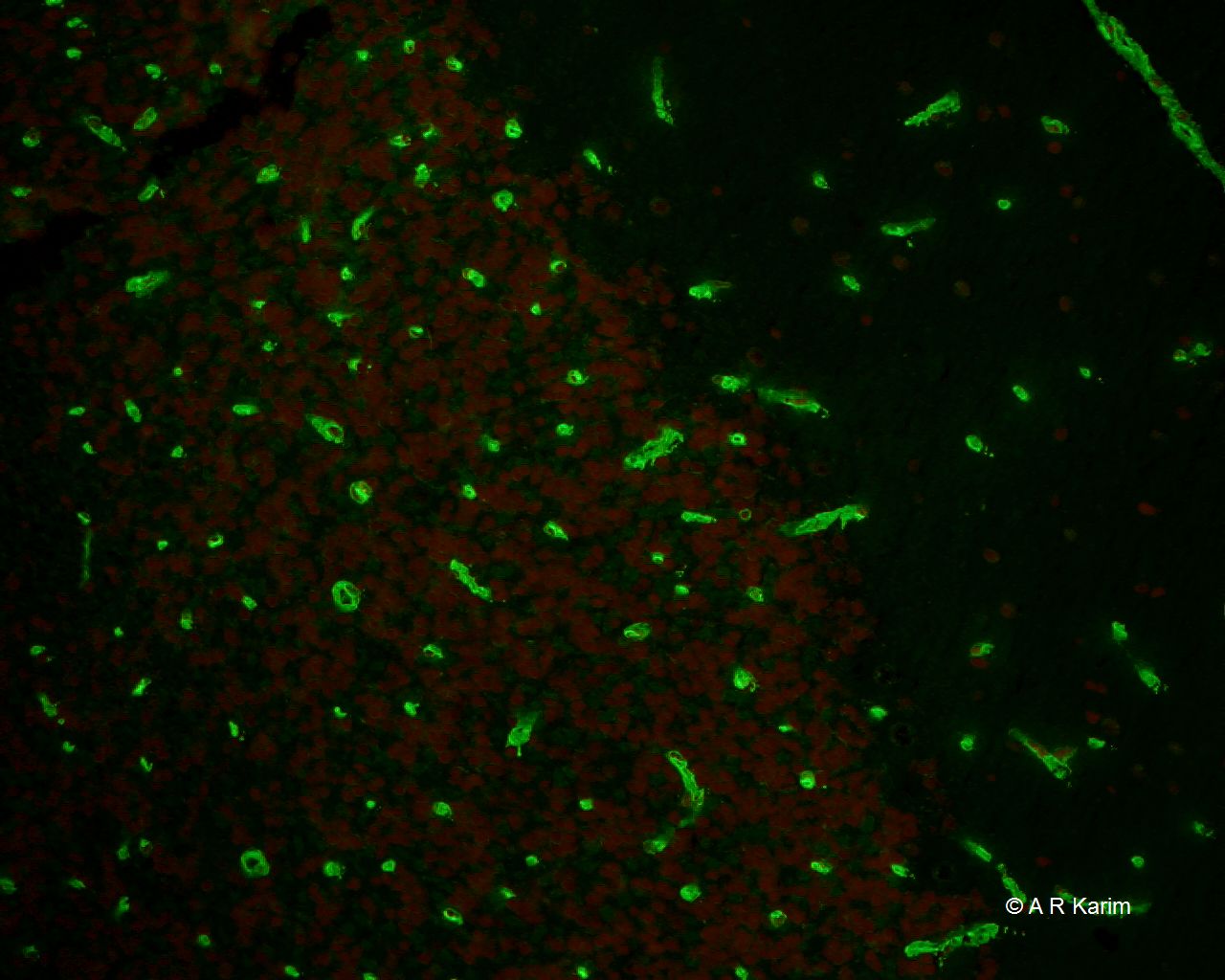
Often, AQP4 antibody is also associated with the staining of the cytoplasm of the granular cells: Such reactivity is also found in the CSF.
.jpg)
Image showing AQP4 transfected HEK cell system considered as having higher sensitivity and specificity.
Clinical: Neuromyelitis optica (NMO, also known as Devic's disease, ~65%) is an immune-mediated demyelinated disorder of the optic nerve and spinal cord. The disorder was previously thought to be a sub-type of multiple sclerosis (MS) but has a completely different pathophysiology. The two can be distinguished from one another by the presence of Aqp-4 antibodies and long segment spinal cord inflammation (referred to as longitudinally extensive transverse myelitis, LETM) which are seen in NMO. NMO is a relapsing and life-long illness and antibodies often remain positive indefinitely.
Treatment is different for each disorder therefore important to distinguish it from MS. NMO is often treated with immunosuppression (steroids, Azathioprine, Mycophenolate etc) and acute treatments often include plasma exchange. Rituximab which is a B-cell monoclonal antibody is used in refractory patients and more recently several new treatment options have been found to be useful in clinical trials These include Eculizumab (complement C5 inhibitor), Satralizumab (Interleukin-6 receptor blocker), Inebilizumab (CD19 B-cell monoclonal antibody) etc.
Glutamate receptor type
Glutamate receptor type
N-methyl-D-aspartate Receptor (NMDAR) antibodies
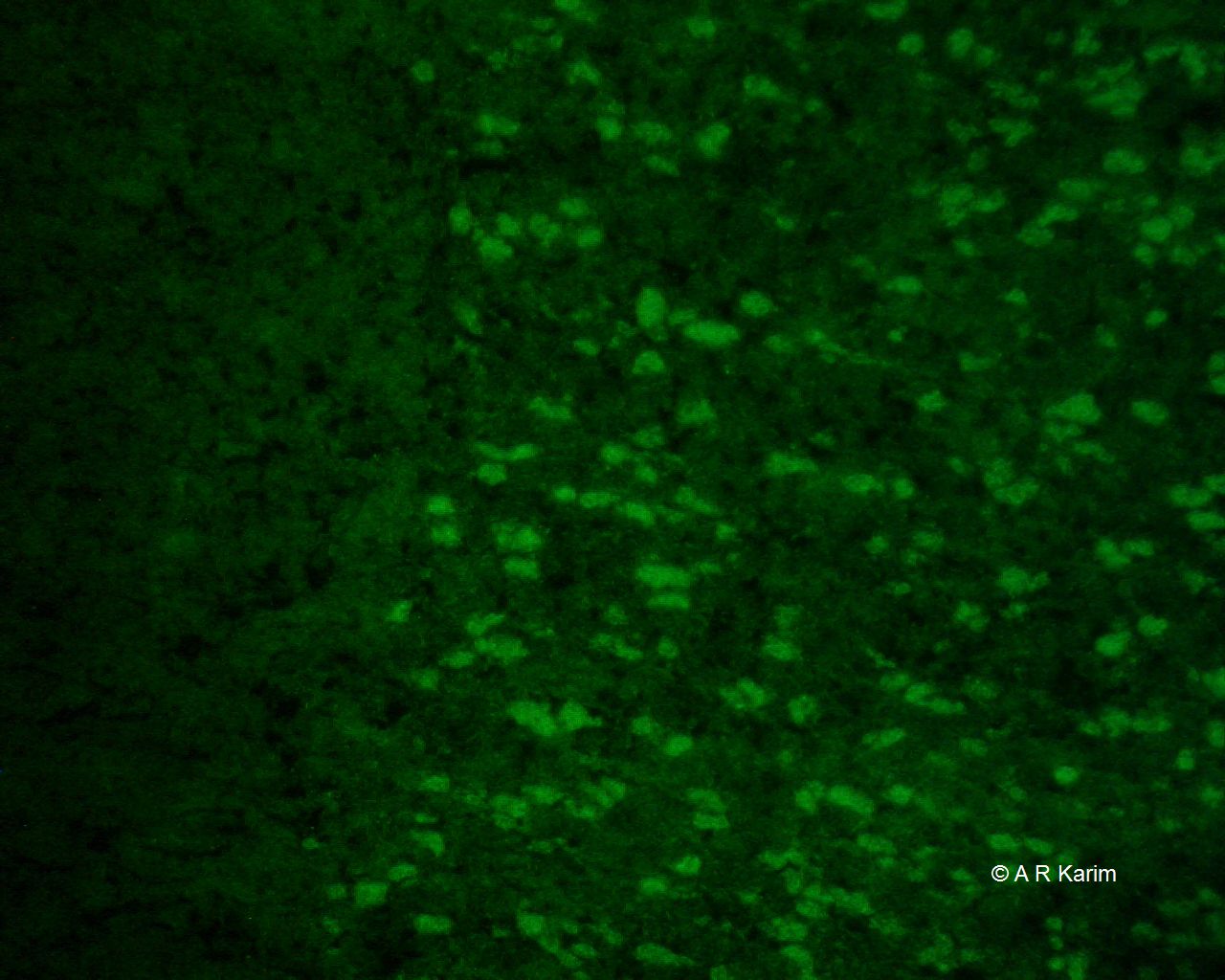
NMDAR antibody is associated with treatable limbic encephalitis and its target is the NMDA receptor which comprises four NR units, with each of the subunit has a molecular size of 100 kDa and together they form an ion channel/receptor. NMDAR antibody binds to the neuropils in the molecular layer of the hippocampus as well as the granular layer of the cerebellum

MDAR antibodies can also be determined using commercially available NR1 transfected cells.
Tumours: Ovarian teratoma (56%, young women).
Syndrome: Limbic encephalitis
AMPAR (alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor)
Tumours: SCLC, breast cancer, thymoma
Syndrome: Limbic encephalitis with psychiatric symptoms
Voltage-gated potassium channel associated proteins
LGI-1 (Leucine-rich glioma inactivated protein 1) antibody
LGI-1 (Leucine-rich glioma inactivated protein 1) antibody
Tumours: Thymoma
Syndrome: Limbic encephalitis with LE with Faciobrachial-dystonic seizures
CASPR2 (Contactin-associated protein 2)
CASPR2 (Contactin-associated protein 2)
Tumours: Thymoma
Syndrome: Limbic encephalitis, cerebellar ataxia, neuromyotonia, Morvan syndrome
DPPX (Dipeptidyl-Peptidase–Like Protein-6)
DPPX (Dipeptidyl-Peptidase–Like Protein-6)
Tumours: Thymoma
Syndrome: Limbic encephalitis with psychiatric symptoms
GABARB1 (GABA receptors 1)
GABARB1 (GABA receptors 1)
Tumours: B cell neoplasms
Syndrome: Gastrointestinal symptoms, weight loss, cognitive deficit CNS hyperexcitability
Diagnosis and treatment of autoimmune encephalitis
There are several antibodies which can give rise to autoimmune encephalitis (see diagram). In our lab this is done as a panel, helping to identify the antigenic target using a single assay. Antibodies are best identified by a combination of techniques (immunohistochemistry and immunofluorescence) to increase sensitivity and specificity. Patients often need immunosuppression, plasma exchange and in refractory patients B-cell depleting therapies like Rituximab (especially in NMDAR encephalitis).

Image description - Summary of encephalitic antibodies
Image description - Summary of encephalitic antibodies
Common clinical features
- Rapid progressive memory deficit
- Altered mental status, including:
- Lethargy
- Decreased level of consciousness
- Personality changes
- Psychiatric symptoms
Antibody-associated syndromes
NMDA receptor antibodies
Associated features:
- Seizures
- Orofacial dyskinesias
- Dysautonomia
AMPAR antibodies
Associated features:
- Seizures
- Refractory status epilepticus
GABAB receptor antibodies
Associated features:
- Cerebellar ataxia
- Opsoclonus-myoclonus
- Epilepsy
LGI1 antibodies
Associated features:
- Faciobrachial dystonic seizures
CASPR2 antibodies
Associated features:
- Morvan’s disease