
Paraneoplastic Neurological Antibodies
The autoimmune disorder of the nervous system linked to an underlying tumour is due to an attempt by the immune system to subjugate the growth of the tumour expressing neuronal antigens. The unfortunate consequence of this results in a rapid onset of neurological deficits known as Paraneoplastic Neurological Syndrome (PNS).
This phenomenon is rare (<1%) and often accompanied by specific high-titre autoantibodies which are non-pathogenic, react with intracellular antigens and represents T-cell mediated response. These are very useful early diagnostic markers of PNS and also, in some cases, underlying malignancy thus facilitating faster diagnosis and earlier treatment with better prognosis.
Management of PNS
Treatment of the paraneoplastic neurological syndrome is primarily the identification and treatment of the underlying tumour. However, in many patients a trial of immunotherapy may be necessary and this can be effective in most syndromes, especially after the appropriate treatment for the tumour.
Summary of paraneoplastic neurological antibodies
Summary of paraneoplastic neurological antibodies
| Antibody | Staining pattern | PND | Associated tumours |
| Recoverin | Retinal photoreceptor | CAR | SCLC, thymoma |
| Yo (PCA-1) | Purkinje cell cytoplasm & axons | PCD | Ovarian, breast |
| Ma (Ma1) | Neuronal nucleoli of the neuronal cells | PCD, BE | Various cancer |
| Ta (Ma2) | Neuronal nucleoli of the neuronal cells | PCD, LE | Testicular cancer |
| Hu (ANNA1) | Nuclei of both central and peripheral neurones | PCD, PEM, SN | SCLC |
| Ri (ANNA2) | Nuclei of central neurones | OM, PCD, BE | Breast, SCLC, gynaecological |
| GAD | Islet cells & grey matter | SPS | Breast, colon, SCLC |
| CV2/CRMP5 | Oligodendrocytes cytoplasm | PEM, SN | SCLC, thymoma |
| Amphiphysin | Central presynaptic terminals | SPS, SN | Breast cancer, SCLC |
| mGluR1 | Purkinje cell cytoplasm, climbing fibre | PCD | Hodgkin’s lymphoma |
| ANNA-3 | Purkinje cell cytoplasm & nucleus + glomerular podocytes | PCD, PEM, SN | SCLC |
| PCA-2 | Purkinje cell cytoplasm and other neurones | PEM, PCD, LEMS | SCLC |
| SOX1 (AGNA) | Nuclei of Bergmann glia of cerebellar Purkinje layer and glial in white matter | PND | SCLC |
| Zic4 | Staining seen in the neuronal nuclei of cerebellar granular layer (but not Purkinje cells) | PCD | SCLC |
| PCA-Tr | Purkinje cell cytoplasm with “dots” in molecular layer | PCD | Hodgkin’s lymphoma |
| Titin | Stains striations in the skeletal muscle | MG | Thymoma |
KEY: PND = paraneoplastic neurological disorder, PCD = paraneoplastic cerebellar degeneration, PEM = paraneoplastic encephalomyelitis, SN = sensory neuropathy, OM= opsoclonus/myclonus, BE = brainstem encephalomyelitis, LE = limbic encephalomyelitis, LEMS = Lambert-Eaton myasthenic syndrome, SPS = Stiff person syndrome, CAR = Cancer Associated Retinopathy. MG = Myasthenia Gravis, SCLC= small cell lung carcinoma, AGNA = anti-glial nuclear antibody, DNER = Delta/Notch-like Epidermal Growth Factor-Related Receptor, SOX1 = gene that encodes a transcription factor with a HMG-box.
Overview of PNS antibodies
Hu (ANNA1) antibodies
Hu (ANNA1) antibodies
| Cerebellum | Rodent stomach | ||
|---|---|---|---|
 |
Hu antibody binds to the granular and Purkinje neurones. | 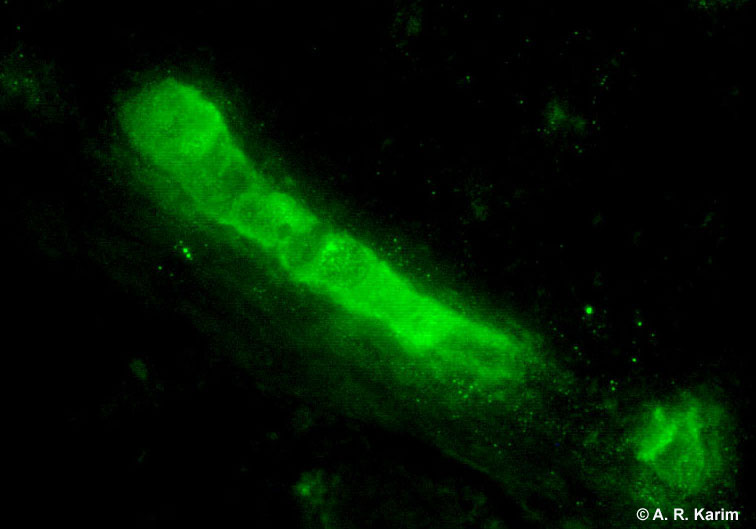 |
Anti-Hu antibody staining myenteric plexus. |
This is the most commonly occurring paraneoplastic neurological antibody.
Neurological syndrome: Cerebellar ataxia, encephalomyelitis, sensory neuropathy.
Associated tumour: Small cell lung carcinoma and neuroblastoma.
Ri (ANNA2) antibodies
Ri (ANNA2) antibodies
 |
Rare antibodies (IgG) Similar staining pattern as anti-Hu antibody Antibody binds to CNS but not PNS neurones (myenteric neurones stain negative) A high intensity signal at both 55 and 80 kDa on a Western blot would confirm Ri specificity. Neurological syndrome: Cerebellar degeneration, opsoclonus/myclonus Associated tumours: Breast, gynaecological and small cell lung carcinoma |
Yo (PCA-1) antibodies
Yo (PCA-1) antibodies
.jpg) |
Yo antibody (also known as Purkinje cell antibody type 1 (PCA-1)) reacts with primate cerebellum with coarse granular staining of the Purkinje cell cytoplasm. This reaction must be confirmed with Western blot/line blot. Note: the red neuronal nuclei are due to ethidium bromide counterstain. |
Clinical indication: Cerebellar degeneration
Associated tumours: Breast and ovarian carcinomas. With only few exceptions PCA are found exclusively in female patients.
Amphiphysin
Amphiphysin
.jpg) |
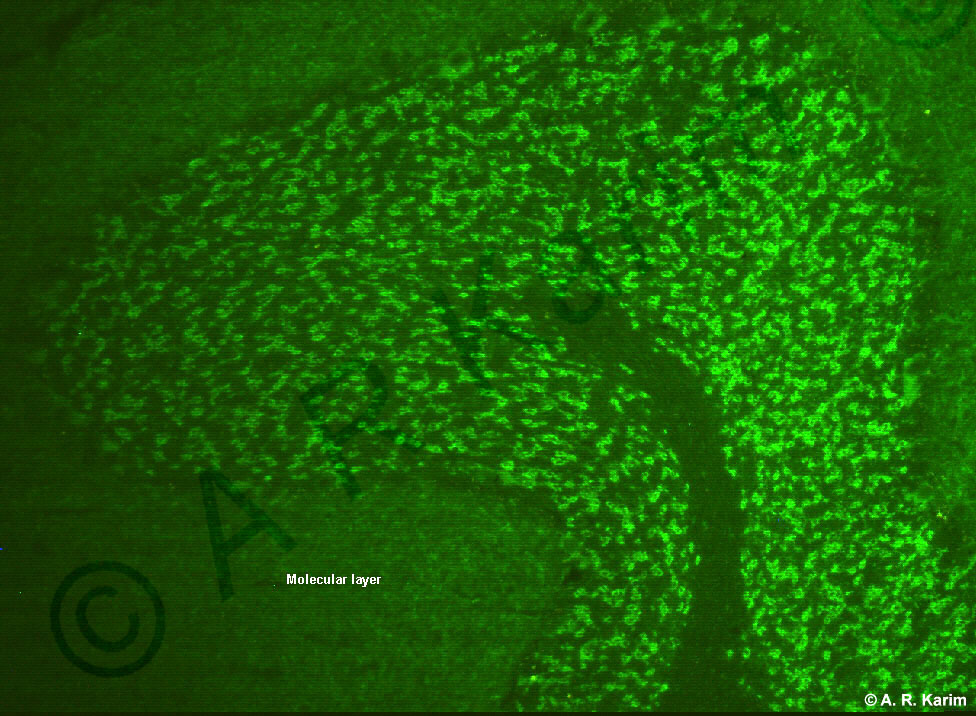
Amphiphysin (128 kDa dimeric, synaptic protein) is found in cerebellar presynaptic nerve terminals. The cell processes in the molecular are stained more intensely than the nerve terminals in the granular layer. The pattern in the granular layer resembles that of GAD. |
Amphiphysin can also coexist with Hu, CV2 or PCA-2.
Clinical conditions: Stiff person’s syndrome (5%), paraneoplastic encephalomyelitis.
Associated tumours: Most common malignancies are small cell lung carcinoma and breast cancer.
CV2 (CRMP5)
CV2 (CRMP5)
|
|
CV2/CRMP5 is a 66 kDa protein found in the cytoplasm of oligodendrocytes in the white matter. |
.jpg)
When this antibody was first described, it was called CV2 and now it also known by its antigenic protein (collapsing response mediator protein 5; i.e CRMP5).
Clinical conditions: Paraneoplastic encephalomyelitis/sensory neuropathy.
Associated tumours: Thymoma, small cell lung carcinoma.
Ma antibody
Ma antibody
Three types are known, Ma1 (Ta), Ma2 and Ma3. These have a similar pattern of distribution on the cerebellum. All three antibodies can coexist with each other and this is reflected by additional symptoms compared to isolated reactivity.
Cerebellum: Ma is located in nucleoli of the molecular and Purkinje neurones. Nucleolar ANA must be eliminated as it produces similar pattern as Ma. This type of distribution can also be seen with non Ma sera of undetermined significance.
Testis: Nucleoli are target antigens for the anti-Ma antibody. Positive testis indicates Ma1 reactivity. Note testis lack Ma2 reactivity. This implies that the above sample contains both Ma1 and Ma2 reactivity.
Clinical conditions: Limbic or brain stem encephalomyelitis
Associated tumours: Testicular, lung
Tr (PCA-Tr) antibody
Tr (PCA-Tr) antibody
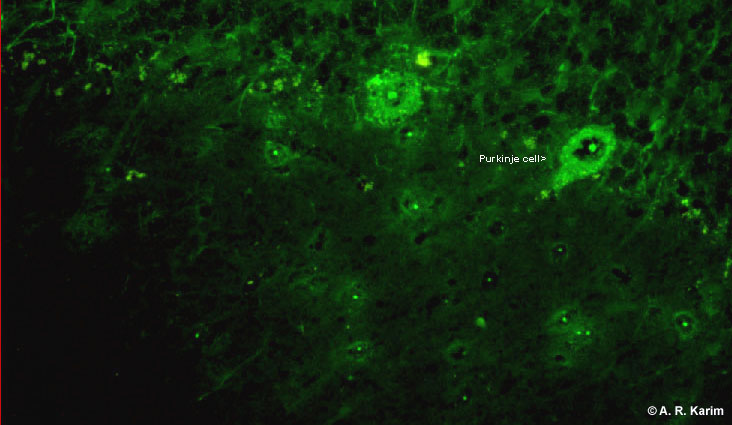
This is another IgG specificity which reacts with the Purkinje cell cytoplasm.
.jpg)
Primate cerebellum: The anti-Tr antibody stains cytoplasm of Purkinje cells together with the dendrites. In the molecular layer, punctate (dotted) pattern distinguishes from Yo. The staining in the Purkinje cells is finer than that of anti-Yo antibodies.
Associated tumour: Hodgkin's disease
Neurological syndrome: Cerebellar degeneration
Glutamic acid decarboxylase (GAD)
Glutamic acid decarboxylase (GAD)
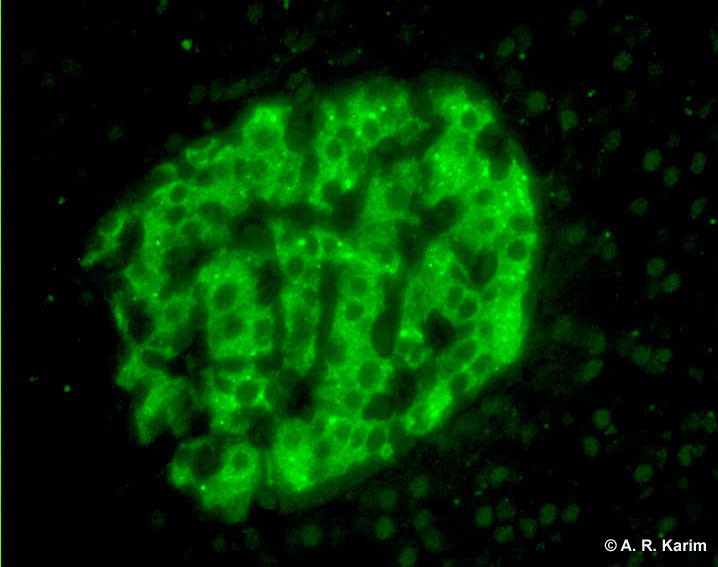
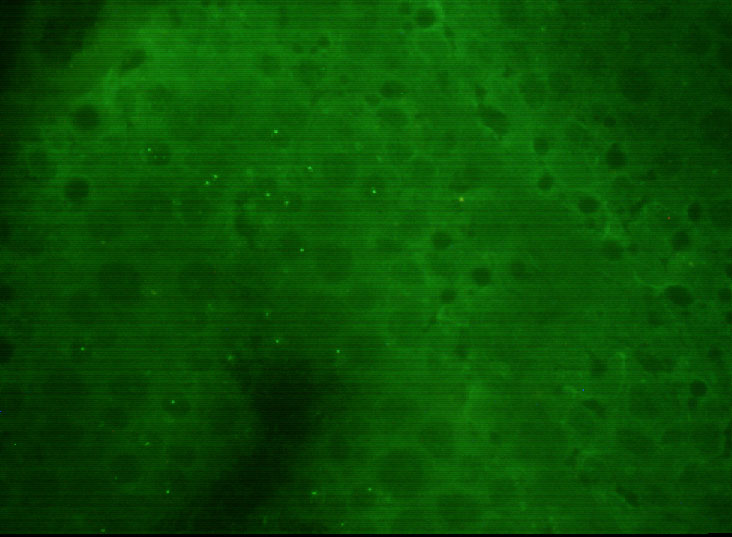
GAD antibody on primate pancreas (Islet cell antibody has similar distribution). The target antigens are GAD 67 and GAD 65 which are associated with Stiff-man syndrome and insulin dependent diabetes mellitus respectively.
Low magnification: GAD staining the granular layer in the primate cerebellum. In contrast to amphiphysin there is a lack of staining in the molecular layer.
.jpg)
Neurological syndrome: Stiff person’s syndrome or diffuse hypertonia. GAD has also been reported in cerebellar ataxia, epilepsy and myoclonus.
Tumour associated: Breast, colon, small cell lung carcinoma
Myelin associated glycoprotein (MAG) antibody
Myelin associated glycoprotein (MAG) antibody
.jpg) |
Primate sciatic nerve showing anti-MAG IgM staining the inner and outer myelin of axons (targets is a 100 kDa glycoprotein). | |
|
|
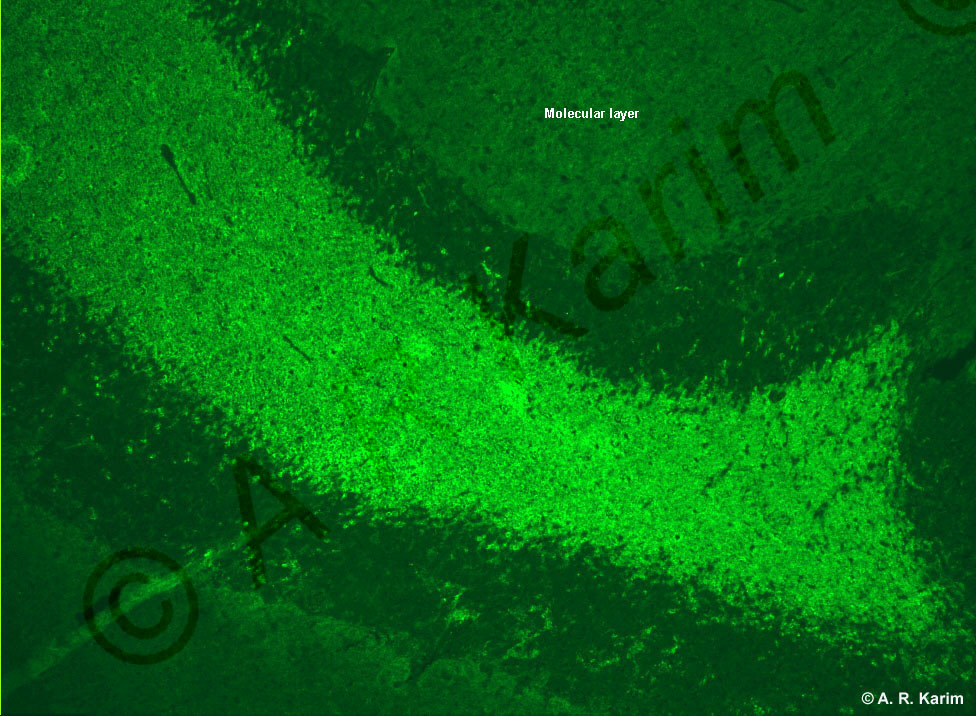
Anti-MAG (IgM) binding to the white matter sandwiched between the granular layer of the primate cerebellum. Neurological syndrome: Peripheral neuropathy Associated tumour: Waldenstrom's macroglobulinaemia, multiple myeloma |
Skeletal muscle antibody
Skeletal muscle antibody
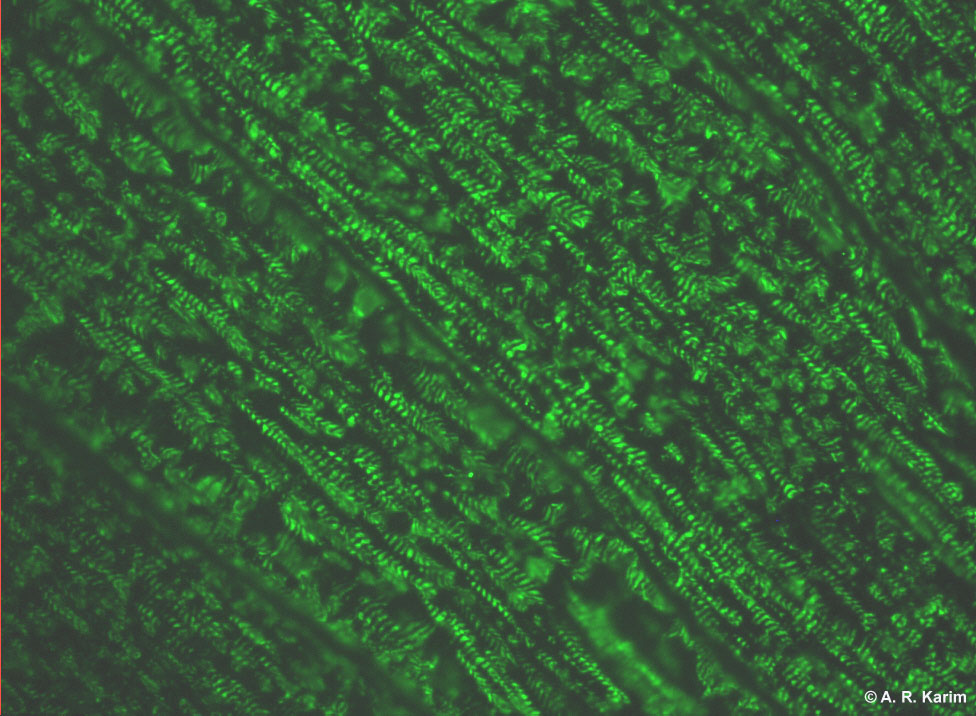
Antigen: contractile elements of striated muscle
Disease: myasthenia gravis
Associated tumour: Thymoma
Human IgG antibody to primate skeletal muscle showing staining of the striation. Compare this pattern with cardiac antifibrillary antibody.
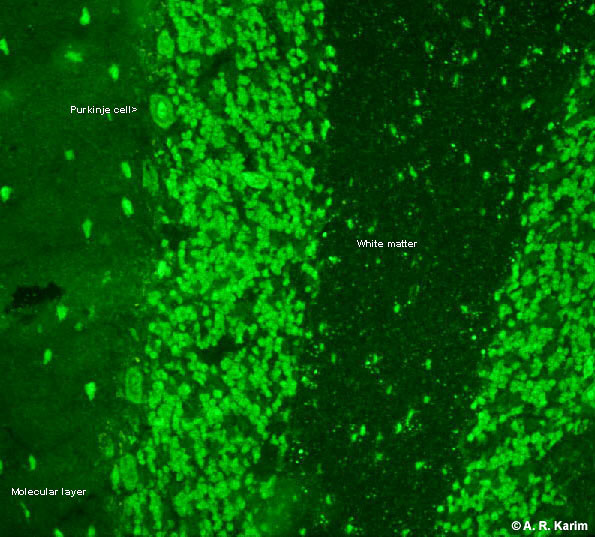
Cerebellar architecture
Paraneoplastic neurological antibodies: For detection of these, it is necessary to be familiar with cerebellar histology.

The cerebellum consists of the white and the grey matter. The latter is subdivided into Molecular, Purkinje cell and Granular layer (contains densely packed granular cells). The Purkinje cells can easily be identified due their large size. These are located on the border of granular and molecular layer. The most favoured method for detection of paraneoplastic antibodies is to screen patient’s serum on cerebellum and any positive reaction producing identifiable pattern is further confirmed by alternative method such as line blot consisting painted recombinant proteins.