The ROTATE study is investigating how best to get babies into a good position for a vaginal birth when problems arise at the end of labour. At this stage, most babies have rotated round in their mother/birthing person’s pelvis so that the back of their head (the occiput) is at the front of the pelvis. This position is most likely to result in a straightforward vaginal birth. But some babies end up in a position where the back of their head is against the woman/birthing person’s spine, or her left or right hip, making it more difficult to push the baby out and more likely she/they will have bad tears and/or more complex late second stage caesarean birth

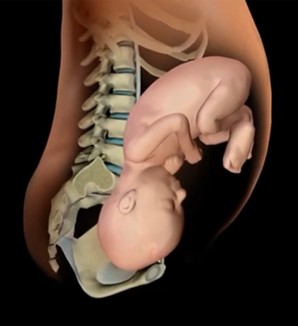
Optimal birth position
Back-to-back position
In this situation an obstetrician (a doctor specialising in pregnancy and birth) will discuss the options and seek consent. When continuing with a vaginal birth, the obstetrician will help turn the baby so their head is in the best position for birth. There are currently two options that are already routinely used:
1. Using their hands to rotate the baby (manual rotation). The woman/birthing person may then be able to push the baby out without further assistance. If not, the obstetrician will use forceps or ventouse to help birth the baby.
2. Using forceps or ventouse to rotate the baby (instrumental rotation) and then to help birth the baby.
Currently, there is no conclusive evidence to say which method of rotating the baby’s head is best. Different doctors use different approaches, which is why we are doing the ROTATE study.
We want to find out which of these two methods is the best for both mothers/birthing people and their babies. We will be collecting information about the outcomes, such as tears and late caesarean sections. Obstetricians generally want to avoid carrying out caesareans in the second stage of labour as they are riskier to the woman/birthing person and baby than those that take place before labour starts or in early labour.